
|
Blog
|
|
The best way to keep informed about my book(s), events, promotions and special deals,
is by subscribing to my mailing list. |
|
|
|
Blog
|
|
The best way to keep informed about my book(s), events, promotions and special deals,
is by subscribing to my mailing list. |
|
|
As a spirited person I love people and like enhancing their quality of life.
My body chronically deals with a variety of debilitating problems. Medical gaslighting has become my concern. I am committed to sharing my story to give other patients the courage, strength and vocabulary to speak up. I believe this will lead to improved communications between patients and professionals, and deeper understanding among the community at large. My book Recognise ME can be bought as eBook and paperback: UK, Mainland Europe, USA. You can also get Recognise ME via Waterstones and Barnes and Noble. Reviews can be left on all of these sites, as well as on Facebook. The more of them, in the more places, the better! Anneke. |
Back to Blog
Colonoscopy.24/6/2024 Do you remember how I spent time in a local hospital in March with pain that was initially suspected to be caused by a kidney stone? It was decided that further investigation was necessary. Gastroenterology was to be the first port of call. I anticipated being brushed off with irritable bowel syndrome or something like that, caused by stress and lifestyle, only years later to find another cause and the recognition and approach that comes with it. It felt important also to be seen by someone who is aware, or at least wants to be aware, of my already diagnosed conditions, and understands the possible interplay of the various factors. I used to know such a specialist. He moved to a university hospital further away, where he now works as professor. After several conversations with my loved ones and with the professionals who support me medically and socially, it was decided to make an appointment with him, if possible. There were consultations available earlier with other gastroenterologists, there and closeby. I was told that to see the professor himself, I would have to wait until May 27th. I chose to endure the severe pain until after our trip to the UK for the launch of Recognise ME, which was scheduled for May 15th in Leeds. The fortnight we spent there proved how well my husband and I are attuned to each other in navigating my body’s antics. With the generous support of friends it turned into a wonderful time. We would return home late in the evening on Saturday the 25th. Jean could go to work on Monday, May 27th, while I would get to the hospital by public transport. All kinds of unrelated issues thwarted our plans, things that were difficult to foresee and that belong in other people’s stories. Still, I made it on my own, by train and bus. Someone working under the professor's supervision recommended a colonoscopy to ensure that everything was fine and, as predicted, pin the pain on a functional problem. I asked him about his knowledge of EDS, and he seemed to know something, in relation to the digestive system. That helped. When I suggested he might check with my endocrinologist, in the same hospital, whether and how my cortisol intake should be adjusted for this procedure, he thought it would be better to make an appointment with the anaesthetist. He handed me the necessary paperwork. As I continued to refer to the original agreement, after a long wait, he accompanied me to the counter to establish that the follow-up would actually be carried out by the professor. It took determination and patience to finally speak to the man himself. He went over everything again in the presence of this junior, from a broader perspective based on years of experience and acquired knowledge. The plan was confirmed. Trying to arrange the anaesthetist appointment, I was sent from pillar to post. Eventually, I was given a questionnaire, several pages thick. Based on my replies it would be decided whether such a consultation was necessary. If so, I would be contacted. The only way I could manage to complete this task, after the day I had had, was by arranging for Jean to pick me up by car after work. We were both at the end of our tether. Last week I was expected in the day hospital. The day before, I received a phone call to ask how the preparation for the colonoscopy was progressing and if I had any questions. I was waiting for the bus after having my intensely painful neck treated. In other circumstances, I might have thought to ask about the cortisol. I decided for myself to stick to my usual dose of dexamethasone. I would be in good hands in this hospital, my endocrinological file is based there. The nurses were friendly and caring. They confirmed that the answers I had given in the booklet had been entered into the computer. When reading it out, they pointed out explicitly that gluten and cow's milk cause an intolerance rather than an allergy. In my case that is correct, although it could have been different. Once I was admitted, I posted a photo of myself in a surgical gown on my Facebook page as part of an ongoing effort to make barely visible conditions seen. I added the words: ‘It's OK. It's only a colonoscopy, under anaesthesia.’  When someone wrote: ‘I hope it goes well and stay assertive there,’ and ‘Don't let yourself be gaslit,’ I replied: ‘So far I have always been treated well here. Hopefully it stays that way.’ After the preparation and some waiting, it was my turn. The same doctor who had originally replaced the professor was on hand. He had to check with his team which procedure I was there for. I found this somewhat perturbing. As far as I was concerned he might as well perform a gastroscopy, though, while I was anaesthetised. Sooner or later it will be called for again, anyway. He stuck to the original plan. When adrenal insufficiency was emphasised again (I insisted on informing everyone who said anything to me - as a patient you learn over time), the anaesthesiologist was taken aback. After some discussion she discovered in the computer that a completed questionnaire had indeed been submitted. That information would have to do. Much later than I expected, I woke up groaning. ‘Madam, are you in pain?’ I realised that was indeed the case and confirmed. ‘Are you nauseous?’ I was. I also mentioned that I felt like I needed some extra cortisol, and again relayed my diagnosis and mentioned the professor of endocrinology in the same hospital, who could confirm this. ‘I have to ask the doctor,’ she replied softly, ‘the professors have gone home.’ The pain relief came, as did something to treat the nausea. ‘I can only administer what the doctor agrees to.’ My request for cortisol had apparently been rejected, because my parameters were all stable. My blood pressure, heart rate, etc. were exactly the same when it came to pain and nausea. If I had complained of itching, I would almost certainly have been given something to deal with it. These are sensations that, I assume, every doctor and nurse has experienced and can therefore imagine. By contrast, only patients with adrenal insufficiency know what a shortage of cortisol feels like. Much as Eskimos have different words to specify types of snow, where we only have one, our language lacks the vocabulary to express the sensations associated with something too small a group ever lives through. And so, parameters are conclusive, over and above the account of the seasoned patient. I was just sharp enough to explain that there is a long distance between feeling optimal and a situation that is alarming, and therefore visible in the measurements. For the first time in my life in this kind of setting, after everything I've been through, I heard myself say: ‘It's my body!’ I was about to leave. In the meantime, someone came to ask me if I preferred a ham sandwich or one with cheese. ‘Are they gluten-free?’ I asked. ‘No,’ was the answer, ‘we can give you yoghourt.’ ‘Without cow's milk?’ Negative. This happens often. It is usually followed by a mild state of panic during which solutions are considered. They will find something eventually. In this case that happened very quickly and peacefully: ‘We can get you some water.’ When I later asked if someone had perhaps been sent to a well to tap it, it appeared to have slipped their minds. I was soon given a half-filled paper cup. ‘Madam, you must stay. The doctor needs to speak to you,’ was followed by, ‘Ah, he's here!’ I had little choice but to listen to what he had to say. A large amount of polyps had been found. He seemed impressed. He had taken a few out, larger ones. The procedure was to be repeated within 6 to 12 months, after consultation with him. The fact that I already have an appointment to discuss the results with my preferred professor, which he himself ensured, appeared to escape his mind. That surprised the nurse, who went to confirm whether my statement was reliable. I also tried to explain to him the difference between a lack of cortisol and an alarming situation. He asked if I wanted methylprednisolone. ‘No. Cortisol, or hydrocortisone, whatever you like to call it.’ He had apparently misunderstood that too. If medrol was the only option, it would offer a solution, but why start with something so strong? ‘Do you have that with you?’ he asked. When I confirmed I did, he shrugged his shoulders. He seemed to swallow the words, ‘Then what's the problem? You're leaving anyway.’ Let's face it, I've been through enough anaesthetics to know how I'm supposed to wake up from them. The distress I experienced could easily have been avoided, read: treated. That would require some knowledge about either the condition or my medical history, preferably both. One call to the endocrinology department could have saved the trouble of doing that research. If for whatever reason, even that was too much to ask, there were only two options left: either trust the patient with more than 10 years experience of living with this diagnosis, and more than 52 years of experience living in her body; or leave her to suffer. He chose the latter. Had I been more alert, which might have been the case if this had been handled correctly, I probably would have asked a few more questions. All I managed was to express my relief that a cause for my pain had been found. ‘Polyps don't hurt,’ he said dryly. Later I learned that that too was wrong. Something sprang to mind that did need to be clarified. ‘Then, why does it need to be followed up further?’ ‘Because it could turn into cancer,’ was his equally cold reply. I was left guessing whether what he had cut out was going to be examined, whether this multitude of polyps indicated something out of the ordinary, whether this occured more often in EDS patients than others, or what the further course might be. Hopefully the professor will enlighten me in August. I try to trust that I will get to speak to him as agreed. Maybe my family doctor can tell me more in the meantime. Otherwise I'll just have to live with that threat hanging over me. I have been down this road several times before. So far I have survived. The big difference in me is that instead of starting to doubt my own integrity and mental health, I see who made the mistakes here. Individually they may have been relatively minor, but together they undermine the otherwise excellent image and reputation of this hospital. The damage caused by the disappointment, the loss of confidence, the accompanying anger and some bitterness, the doubt and fear, well, I can contact my psychologist about that.
0 Comments
Back to Blog
Delay.18/6/2024
First let me apologise for this blogpost being late. A number of factors combined made that happen.
Shortly before we left for the UK to launch Recognise ME, I called my neurologist’s department to cancel the bone scan and the appointment with him to discuss its results. My neck was fine. I should have known that would tempt fate. It started threatening to play up a bit, but there was little to be done about that. I considered a visit to our family doctor to ask for another course of anti-inflammatory injections. They helped well before. Then it started executing its threats. I self-diagnosed subluxations, and did what I could to deal with them. The more experience I gather with chronic illness, the less any physician gets to see me. What I said many years ago to Dr. O, my family doctor at the time, still stands. If I turned up every time something went wrong, I would have been there every day. Instead, thanks to his and many other professionals' insistence on finding patterns and ways to deal with them, I have a whole host of coping strategies to handle various things most people would hurry to an emergency department with. So, I dealt with it when I injured my neck worse last Sunday morning. It was a stupid thing to do. It could have been avoided. I dropped my spectacles between my bed and my bedside table. I could have gone for the easy reach. I could have rolled the bedside table out, my husband did put wheels under it for that purpose. I could have asked him to pick them up. Instead I turned over and reached down awkwardly, and howled as I retrieved them. My spine was frozen still from the atlas down to my shoulderblades. I went from having been able to get up and prepare breakfast, to being completely dependent and bedbound. It was a case of waiting to see what would happen. As the day progressed I experimented gently, pulled various tricks out of my hat, and managed to get the situation to improve somewhat. Meanwhile I was already preparing for the colonoscopy I am having done under anaesthetic tomorrow. Because my digestion is known to be slow, as with many EDS-patients, I started the very restricted diet early. Tonight the real emptying starts - oh joy! It might all prove worth it, if a treatable cause can be found for the pain I have lived with since my last hospital admission, where a kidney stone was initially thought to be the culprit. By late afternoon, I allowed it all to get the better of me. There were other things bothering me, too. My next 50 paperback copies should have arrived last Tuesday. I was waiting to hear from my publisher what had happened to them. I had had to tell people they would have to wait. In itself that is a positive, of course, there is interest in them. Still, I felt embarrassed and frustrated. With a bit of luck the order has being put through today. On the internet, the paperback orders are slow. They are happening, about one every other day. Again, there is good news in that. It put me in my place, though, as I had started blowing my own trumpet to myself. Humility, while I have had a lot to say about it, pertaining to other people, I could learn a thing or two about it myself. Still, I looked for opportunities and solutions. I made a reel to illustrate why the kind of conditions I live with are rarely visible. The sight of me in agony, hardly able to move, is what my husband, our son, and exceptionally a few others who are very close to me get treated to. The rest of the world sees me at my best only. Perhaps as a community of patients we should share these occurrences more often. Maybe then we might get over it needing so much courage, and emotional as well as mental effort to show what our lives are like. I tried to dictate to my chromebook, and failed. That is when I cracked. I gave in. I considered you might all survive if I postponed writing and posting something for my blog. Who was waiting to read it anyway? It sent me in a negative spin. I allowed myself to lose confidence, in everything there is to say about me. Most of all it undermined my belief that I can and will continue on the path of rehabilitation, with all its up and downs, let alone make a positive difference to anyone else’s life. That scared the living daylight out of me. Yet, here I am, back on track, shaky as that may be. What happened? Time, and an acceptance that I needed to go through whatever came over me, shifted my mood back to something I could cope with. More importantly, though, I received another five star rating on Amazon. Later the review that belonged with it came too. Something else also happened. In response to Lupus and Me posting about The 5 Types of Lupus Fatigue, I shared an excerpt from my book. "In my younger years, all I had known was that I was permanently done in. Now I developed a vocabulary to explain the nuances of my tiredness. My lifelong fatigue dragged on. It was as if the feeling itself sapped energy. Imagining doing anything took too much effort. At its worst even breathing appeared to require deliberate focus. It was hard to tell what influenced it. It could simply be how ill I still was. The change in diet might play a role. My level of activity had some effect on it. So did the drips and the amount of time in between them. Much as lack of energy was present in depression, it existed independent of it too. Natural emotions played a role. Guilt, uselessness, anger, disappointment, grief, and the like, could be the effect as much as the cause. It looked like a lack of motivation and confidence. In truth, I was always full of ideas and a sense of responsibility. I still spent nearly all my time in bed. On the other hand, I was awake more. Most days I was up for a short while. I pulled up and let down the blinds myself. Still, it amounted to very little. There were many things I wanted to do. Whenever I recovered a little, I would go all out. As a result, most days I ended up lying in bed recuperating. I slept. I watched television. When I felt slightly better I played around on the computer. Food was brought to me. I made it downstairs to have my drip, which offered a plausible excuse to lie about for several hours. Afterwards I returned to bed. The interactions with the nurse were enough to leave me washed out. With any kind of infection, my enthusiasm did wane. Another type of weariness took over. The zest was gone. It was replaced with dread and heaviness. It would only pass when the microbes had been dealt with. Eventually, staring into infinity was the only option left. It was numbing. For those close to me it was as frustrating as it was to me. The best way to handle it was to let it be. When it was ready it would leave. I had received ample criticism for giving in to such complaints. Against better judgement I would keep pushing myself. The balance between rest and activity was always delicate. Walking a tightrope might have been easier. When I got it wrong, there were consequences. My whole body was sore the day after a stroll through the park in the wheelchair. Despite the stiffness and spasms, I still had a sense of achievement. A pattern appeared whereby I started the day feeling lethargic. A little more activity was possible by afternoon. This was followed by a lovely, very deep sleepiness in the evening. Jean was moved to hear me mention having earned it. Mornings and evenings the pain would travel through my body like a cable car. It was difficult to handle. As I started to recognise this sequence the promise of adventurous afternoons got me through. Gradually I became more audacious. The occupational therapist who had given her advice when we were looking for a new school had become a good friend. She had two boys of around the same age as ours. She took me and our young, erratic jesters to a local funfair. She pushed my wheelchair. The joy, laughter, hilarity and natters left me thrilled. I envisaged steadily building up my strength and stamina. When I pushed my boundaries too far, devastating exhaustion set in. My most productive days left me worn out. I wanted to concentrate on everything and nothing. I seemed fuelled by adrenaline. It was like having drunk too much coffee. It rendered me wide awake, but void of vigour. Overstimulation was the word. Every minor signal entered my consciousness at full blast. Sleepless nights were more often caused by a shortage of vitality than by abundance. Instead of rejoicing in my accomplishments, I regretted my escapades. Panic struck. What had I done? Why? How bad would this get? How long would it last? What else should I expect? How could I avoid this in future? I went as far as fearing for my life. I had regained a taste for it. I wanted to live. It was understandable the psyche was considered when a patient kept complaining of listlessness and general aches and pains. It should be. In my case, there was now proof my body was responsible. Yet, I kept myself under scrutiny. I looked well. I should be coping. I clearly failed to. That was down to me. I had to change. My OT training had covered sleep hygiene. Applying this method should result in a healthy level of vivacity throughout the day. Rhythm was key. Wake up and go to bed at set times and stick to them. Only use the bed for sleeping. Stay out of it at all other times. There was a lot more to it. It had always been torturous to me. I had tried it. I felt obliged to. For years I followed advice that increased my suffering. My husband and I decided I would stick to my own rules. I would sleep whenever my body wanted to. If I was alert during the night, I could use that time productively. I paid bills. I saw to correspondence. I read a little. It worked much better. Taking it gently, day or night, was the only answer. Otherwise restlessness left me hanging between sleep and wakefulness. The trick was only to do easy things, briefly. In between those, I had to recover. My body and soul would take over and start doing something again when they were ready. That worked well in theory. In practice this regime was hard to follow. A lazy day once in a while allowed for a pleasant kind of doziness. In contrast with most of the above, it left some spark available. It was easy to give in to. It was pleasurable. In fact, I often got more done. The pressure was taken away. Only fun tasks were undertaken. They counted. Our boy asked me what the word lazy meant. I explained as best I could, in terms he would understand. In bitterness and humour I added, ‘It is like your mother.’ Within a fraction of a second he answered, ‘Mummy! You are NOT lazy! You are ILL!’ This little fellow could see what countless professionals had missed." I repeated it in answer to the Ehlers-Danlos Society’s question what fatigue feels like. The responses there were fast and strong. My writing was described as superb, well-written and so true. I am being thanked for explaining our daily struggles to the world, in words others have difficulty finding. It reminded me of a particular review sent to me by one of my advance copy readers, who has previously appeared here as guest-writer. ‘As I was reading Recognise ME, what struck me again and again was the amount of detail and nuance expressed in relation to what it is like to be in our "spoonie" "striped" skin. Many people write and talk about exhaustion, pain, shame, and guilt when they write and talk about chronic illness, chronic pain, and being disabled. Anneke writes about all of these facets, yes. But more than that, Anneke writes about our lived experience in ways that generate far more understanding and empathy than I thought possible. When I read passages of Recognise ME to the abled others in my life I could see the light bulb turn on. I could see comprehension and compassion spread over their features. They would gasp and tell me that NOW, they "get it". This effect proves Recognise ME to be invaluable. For how else do we change our world for the better if not by increased understanding and empathy?’ Adam Lodestone Mental health professional who is also a fellow EDS Zebra, writer, and advocate. It all helped to get me back in the saddle, albeit metaphorically only. It shows the importance of strong and positive responses and reviews. On my own it would have taken a lot longer to dust myself off.
Back to Blog
Diagnosis.9/6/2024 ‘How long did it take you to get an ME/CFS-diagnosis?’ is a question I have seen and heard among patients a fair bit lately. Once it was clear other conditions could explain my symptoms in ways that made more sense, I took some distance from that community. It was too painful for me to see others going through similar abuse as I had gone through, and stop myself from screaming, ‘Find other answers!’ What felt right for me, might be entirely wrong for them and vice versa. Having written my memoir about medical gaslighting, I was nudged gently back in that direction by my publisher, Becky Warrak from Raven Crest Books. I contacted various patient support groups. In preparation for a virtual talk to ME support New Zealand, I was ready to find recognition in my answer that it all happened very quickly. The opposite was true. Apparently for self-diagnosing patients across the Western world it takes years, to their great frustration. In the early nineties, I too had taken an article I had read about ME to my GP saying this must be what was wrong with me. Within a few weeks an authority in the field had ordered and performed a host of investigations, in line with the scientific biomedical knowledge at the time. He felt everything pointed in that direction, but more research was required to give anyone a firm diagnosis. It seems in that respect little has changed. The diagnosis is mostly still given on the basis of the medical history the patient presents with and elimination of anything else the doctor can think of. That is where the problem I see lies. As Mama Chill recently said in her podcast with Daniel from Post-Exertional Mayonnaise (worth watching!), I also believe the diagnosis is often given to anyone with a chronic, barely visible and fluctuating condition that fails to respond to treatments which would in most other cases be effective. In mine, there were physical indicators that clearly pointed towards ME, or post-viral fatigue syndrome, as it was called in one of my reports by the same specialist. Of course, when the cohort that is being researched is an amalgam of people with a mixture of yet to be correctly diagnosed conditions, the results will be flawed. The more I learn about the scientific developments, the more I consider it may still apply to me. Many difficult to treat chronically ill patients find they have a combination of conditions, each with their own markers. So, I am in two minds about self-diagnosis. It took about twenty years, and a deterioration that brought me close to death, before adrenal insufficiency, lupus and later hEDS (hypermobile Ehlers-Danlos syndrome) were identified. Each of them equally gave reason to my most obvious symptoms of fatigue, ever changeable pain and mysterious comorbidities in almost every system in my body at one time or another. The difference lay in the fact that in combination, they fully explained what had been going on in my body since childhood. My EDS-diagnosis also came after a fellow patient had voiced her concerns about how similar our issues were. As I had an appointment at the genetics department related to my endocrinology problems, anyway, it was easy to ask the question. It cleared up all the unanswered questions. The change of approach that came with it, has improved my quality of life immensely, despite the fact that 'You will have to learn to live with it' is still the main advice. Would it be fair to expect doctors to be aware of every medical condition, including the more than 1200 rare diseases? Hardly. Things will be missed. Let us accept that. However, apart from perpetual questioning of my integrity and sanity, neglect came with the terms ME, CFS and ME/CFS. Any problem I presented with was easily brushed under that carpet, when it should have been looked into further. It caused much suffering, and nearly cost me my life. Those who are interested in the details, can find them in my memoir about medical gaslighting, Recognise ME. Since it has been considered to have been a misdiagnosis, I have gained significantly more respect and am trusted as an equal partner in my own health care. When physicians are prepared to acknowledge their limitations, in knowledge, experience and resources; something changes. Many patients with lingering, hard to explain symptoms, will do their own research - or will get someone else to. They often know more about what is going on in their bodies, they have had the time to think outside the box, and check and double check what they have learnt, from science and from each other. When that is heard and respected, when that depth is combined with the breadth the medic can offer, discoveries are made. If that fails, at least there is a partnership in which that frustration and sorrow can be shared. Rather than blame and shame, the best symptom-based care available can still be delivered. Regardless of diagnosis, every patient should have a right to that. That is the very core of my message. That is why I wrote Recognise ME, went through the publishing process and am prioritising my energy towards promoting it. 
Back to Blog
Lupus.2/6/2024  The launch of my memoir, Recognise ME, took place on the 15th of May. I chose that date for its symbolism in being our son’s 18th birthday, but also as it was the middle of awareness month for both ME/CFS and EDS. These two conditions play a major role in this book about medical gaslighting.
So do a few others. I had questioned myself whether focussing on the above two was the right thing to do. When I saw a post about lupus awareness month, mistakenly thinking it referred to June, I was relieved. This meant I could now reach out to that community and support their efforts too. My knowledge would need to be brushed up to be able to do that, though. It got lost in the chaos of getting adrenal insufficiency stabilised, and dealing with the effects of the late discovery of hEDS. Those caused multiple hospital admissions, often via the emergency department, and various operations. Meanwhile we were trying to raise our boy, who shared some of my health issues, and more. I was diagnosed with lupus shortly after adrenal insufficiency had been discovered. It was used as a generalised term. The ANA levels in my blood were high. The same indicator had previously led to a mention of rheumatism. Both are auto-immune conditions, in which the body’s cells are under attack from its own immune system. It is reasonably obvious this leads to the patient feeling very ill. As I understand it, firm specific diagnosis would need further investigations. The treatment was likely to be similar, involving immuno-suppressants. Given how complex and intense my case already was, I was all too happy for those to be started on the basis of what we knew. Once my health stabilised, I was able to reduce my intake, and eventually I could leave it out altogether. A rheumatologist told me it was possible to have had lupus and healed from it. My theory has always been that I had become so ill that my body would have tried anything to save me. Fighting against itself must have been one such strategy. As my health was managed better, the need for it disappeared, regardless of what terminology was used. So I have felt like a bit of a fraud amongst lupus patients. What I do know, though, is that it is another condition that can cause deep levels of exhaustion, and chronic pain that changes in location and pattern. It is often late to be diagnosed, and many patients have a history of being medically gaslit before, and some still after diagnosis. That is enough for it to deserve some attention. As soon as I looked into it, I discovered May was the time for action for this condition too! I missed a beautiful opportunity. I apologise, and will do my best to put that right. Photo by Ray Hennessy on Unsplash.
Back to Blog
Return.26/5/2024
There we were, in Dover Port, waiting to board, and I was thinking.
What a fabulous time we have had during our trip to the UK, from day one. It was a journey full of reminiscence and nostalgia, whilst creating beautiful memories to look back on later, and the launch of something new. We met up with wonderful people, old friends and new. We had fun and meaningful connections with random passers by. There was joyous celebration, but also the sharing of pain and suffering. I was deeply touched by the trust vested in me by people who have been close to my heart as well as some who were strangers to me minutes before. My body behaved amazingly well. I am thankful for it. We must have gotten the balance right. We spaced out everything related to the launch of Recognise ME well. That allowed for socialising and sight-seeing according to the rules my physical being sets out. It is something we have learnt and practiced in the past few years, a bit late considering I am now 52. With the right support I could have reached this level of functioning a lot earlier, regardless of diagnosis. The difference lay in the attitude of doctors, therapists, nurses and the like. I now have a team who believes me, believes in me and treats me with respect and dignity. The results are tangible. That is my wish for every patient. That is where my passion in writing the book and getting it read lies. It seems to have become infectious. During the launch as well as the talks that followed to Quaker Friends and to staff and students at the University of Leeds, I could see people listening with intent, gaining insight and jumping on board. For me, the plea in the title of my memoir Recognise ME has taken root. I am trying to navigate the path to being humbly confident and confidently humble. I have certainly received recognition, and I feel fellow-patients have too. I have heard from them in question and answer sessions, and privately, and their stories have touched me deeply. They give me the drive to carry on, to speak for them as requested, until they find their own voice. My vision that the community of patients with chronic, rare, barely visible and/or fluctuating conditions gets a better deal is gaining momentum. I have joined the chorus that has been working towards this for decades. Their chants have too often fallen in deaf ears. The more we sing together, the more we are likely to be heard. There is something miraculous in being part of that, which is hard to describe. Still, the effort involved takes its toll. It has been important for me as well as my husband, who also functions as my main carer, to ensure we looked after ourselves. We have been well-supported in doing so. Another reason to be intensely grateful! We leave with memories of warm connections and beautiful places. Some of them I can share with you via pictures and videos.
The launch can be watched in its entirety on my YouTube channel. That does mean you might want to skip through the parts that should have been edited out. If anyone is up for some volunteering with things like that, I would love to know.
Part of me feels a need to apologise for skipping a blog piece last week, for keeping facebook posts and responses to those of others to a minimum, for putting some answers to mails and messages on hold. Another tells me it is ok. I can feel you all understand and support the way I have set my priorities to be able to meet the highest demands.
Should you like to be kept informed, remember the best way is to make sure you are on my mailing list.
Back to Blog
Achievement.12/5/2024 It has been an emotional journey, our trek to the North of England from Belgium. We have arrived safely, and are both beyond exhausted. So I am keeping it brief. The ride off the ferry and onto the island in Dover was the most overwhelming moment for me. I was filled with a sense of achievement, about our arrival in England and everything that meant. That is a lot! I was also aware of the many sacrifices that have been made to get to this point. The ones so lovingly made by my husband moved me the deepest, as he continued to make them on our way here. His answers was simple, ‘It goes both ways’. He is right. It does. Back to achievement… Back to acknowledging my worth and our worth, alongside mine and our weaknesses and the way we continue to overcome them. This afternoon I checked Amazon again. Those rankings, they are worse than my scales. I know better than to keep going back to see how I am doing. When Becky, my publisher from Raven Crest Books asked me over a year ago how big my dream was, Amazon rankings were the furthest thing from my thoughts! Improving the lives of patients who have been and/or are being medically gaslit, that dream was and remains huge! And yet, every day, several times, I go and see what number is attached to my book. Becky has advised against getting caught up in it. She mentioned algorithms and such. Our son explained how they worked and how the amount of sales have to keep multiplying. I had seen me drop out of the top 100, and watched the figures get worse and worse. When I opened the site, my expectations were low. I was bowled over to see that in one night I have jumped to the highest place I have been ranked since keeping my eye on it. Recognise ME is now at number 21 in the category Hot New Releases of Biographies of People with Disabilities.  THANK YOU! KEEP IT UP! The 99p offer for the eBook pre-order stands for another couple of days. Make the most of it! I will leave you with a few pictures of the last couple of days. They show an inkling of what the term fluctuating disability or condition can mean. It is also often referred to as dynamic disability, which I feel makes it sound too energetic for the conditions it tends to relate to. I am taking a risk making this visible. I am doing it as part of the overlapping international ME and EDS awareness month of May. Wednesday is publication day. You are still very welcome to join the celebrations in the Bobbin Room in Farsley, Leeds from 8pm. Please, register here, so I know you are coming. There will be a live stream on my YouTube channel. I will be posting the link on social media and to my mailing list. Make sure you are on it.
Back to Blog
Itinerary.5/5/2024
The countdown to our trip to the UK to launch Recognise ME has started. We are leaving on Friday.
It is exciting! As usual we have had to organise this expedition carefully, bearing in mind limited energy and financial restraints, as well as necessary adjustments around both our health needs. That means we are spreading our journey to Leeds from Brakel (in Flandres, Belgium) over three days, making use of the cheapest ferry and suitable airbnb accommodations. Once there, we can recover for a few days before the big event. Emotionally it certainly feels big! What an achievement to celebrate, and how… The evening will be supported musically by my friends Robin Fishwick and Kwame D who is currently reading my memoir to inspire tailored songs. My publisher, Becky from Raven Crest Books will share her experience of working with a chronically ill writer with rare disease and fluctuating levels of functioning, and how she ended up advocating for the cause. The responses of the first few readers will be read, as well as some excerpts from the book. There will be a chance to ask questions, and to top it all off, we will end with a quiz. Obviously there will be refreshments. We are bringing Belgian chocolates, and quintessentially Belgian biscuits to tempt you, and as there may well be people with dietary restrictions, we will provide healthier options too. Of course we will bring paper copies of Recognise ME available to buy should anyone wish to. If any of you are crazy enough to want my signature, I will be all too happy to oblige. 
Against all rules of PR and marketing, I have decided to share my worries about it with you. Having booked a room, I have a number to work towards. If few people turn up I fear it will go down like a lead balloon. But what do we do if there are too many? I want everyone to feel welcome! That is why I have been sending out the invitations in stages, widening the group gradually. Though there has been plenty of interest expressed, and intent to come along, it has been hard to get firm commitments. I keep asking people to spread the word in any way they can think of, as I keep doing myself, asking for confirmation. They have responded positively in doing so, but still, I am left wondering if anyone will turn up. So, please, if there is anything any of you can do to reassure me, it would help me save some energy which I am currently wasting on fretting about it. There are still spaces available. Anyone with any interest in the plight of patients with chronic, rare, barely visible and/or fluctuating conditions is welcome, as is anyone who simply fancies being part of this celebration. Please, spread the word, share the invitation and let me know how many are coming, so I can send entry tickets. 
For those who would prefer to watch what is going on from a distance, there will be a live stream. The details of that will be posted later. If you are interested, please let me know, so I can ensure you receive them. Spread out over the rest of our stay, with plenty of recovery time in between, I have several talks booked in. I am looking forward to each of these, and am fascinated by how they reflect the different angles the core of my message can be approached from. As an alumna it is a great honour to be asked to speak at the University of Leeds about my lived experience writing a memoir about medical gaslighting. All faculties are invited to an online, and an in-person presentation. We preferred this to a hybrid meeting, to avoid some of the well-known technical issues that tend to interfere. To Quaker Friends I will be raising awareness about this injustice that is rarely mentioned and of which little is known. Annette Leonard, writer, speaker, and wellness coach, who knows about living with pain and illness as a constant companion, is interviewing me for her Chronic Wellness podcast. Meanwhile the eBook is already available in pre-order from Amazon for 99p, 99c, or 0.99 euro (depending on where you are buying it from). Those sales help me gain visibility, by pushing me up the rankings. Imagine if this would become a bestseller! So, please, consider buying one in support of my efforts. Considering the responses I have received so far, I am reasonably confident in saying you will get something out of reading it, if you do. It is a good book! 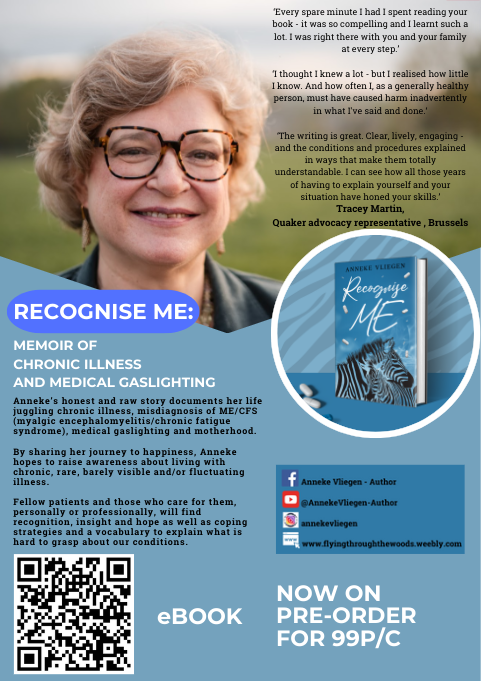
Back to Blog
Pa.28/4/2024 Anyone who has ever met my father, Herman Van Bostraeten, knows that, when he writes a detailed book review, he does it as objectively as possible. The idea that anything his daughter produces, is by definition excellent, would be insane. As such, I am intensely proud that ‘our Pa’ - with his background as historian and archaeologist, once representative of the NFWO (National Fund for Scientific Research), later teacher at the Saint Barbara's College in Ghent, Belgium and also author of multiple articles for scientific and cultural magazines and of his book ‘De Merovingische begraafplaats te Gent – Port Arthur en de nederzetting Sloten’ (The Merovingian cemetery in Ghent – Port Arthur and the settlement of Sloten) which was awarded the Pro Civitate Prijs voor Geschiedenis van het Gemeentekrediet van België (Pro Civitate Prize for History by the Municiple Credit of Belgium) in 1966, and published by this organisation in 1971 - wrote (read: typed) the following considerations about ‘Recognise ME’, my memoir about medical gaslighting, which is to be published on the 15th of May by Raven Crest Books. Anneke VLIEGEN, Recognise ME. A book review. In truth, it has been years since I read - both in form and content - such a rich, complex and layered book as Anneke Vliegen’s Recognise ME. The subjective - what else could it be? - memoir of this author appears, upon critical reading, to be a report, as objective as possible and chronologically structured as it should be, of her evolution from carefree child into adult, spouse and mother, for decades a victim of medical gaslighting. This term - also used in medical circles - means (roughly speaking): if we, scientists, are at a loss about a condition, then it most likely resides in the patient's mind… (As if that would provide a reason to stop searching and helping…) This account of an ever-present battle to survive honourably with a chronic illness, and the considerations of the writer about her own position and behaviour in addition to those of her entourage - reads as fluently and is as engaging as a Swedish thriller: a surprising story full of twists and turns, as unpredictable as the patient’s condition itself.
These questions would be pointless, should they fail to point towards clear answers, or at least to relevant reflections:
The answers have never been formulated. Has anyone ever given them any thought? If so, it’s likely to have been the victims of the lack thereof, rather than those within the circles that could/should (want to?) implement change… These deliberations alone lead to appropriate and applied social criticism… In Recognise ME clear examples are presented. Are politics about steering government towards prosperity and - even more important - towards communal well-being or are they about the battle for power to be allowed to make that happen? And does that work within our, the Western world’s, ideological model? Or elsewhere? More questions than answers. You won’t find the latter in this review, anyway. And who is going to disapprove of that? One thing is clear. ME and chronic conditions in general, form part of a societal context, and create tension between the individual and their environment, between those close and involved and those further away and indifferent. The art to survival is dependent on developing enough self awareness to keep adjusting to the ever changing situation, based on experience and introspection on the one hand, and on the other creating a sizeable and strong enough network of medically and therapeutically trained, nursing and caring, committed professionals, forming a cooperative multidisciplinary team. But doesn’t the most important factor remain the support and understanding of friends and Friends? The answer can be found in the question. Recognise ME is not only a memoir, it is also a bittersweet book about hope and love. In the end light will need to enter the tunnel from the outside; meanwhile there is clarity on the inside through growing individual radiance and that of a sympathetic environment in various areas. This review is certainly no mirror to Recognise ME.
Anneke herself has suffered this culture shock twice, once upon her arrival on the island and years later when she returned to Belgium… There are worse things to worry about! Life as it is, with a smile and a tear… Herman VAN BOSTRAETEN Özdere (TR), 25 april 2024 Recognise ME is already in pre-order as eBook.
Back to Blog
Scales.21/4/2024 Pain
On Facebook and Instagram I run a weekly section on what helped me in terms of medical gaslighting. That led to a discussion about describing pain. There is some frustration among patients and nurses alike about the use of pain scales. This is a common way to establish the level of severity a patient is experiencing. At its simplest, it consists of the question ‘What score would you give your pain, between 1 and 10?’ Sometimes visuals are added, consisting of colour gradients from green to red, happy to angry/hurt faces, or rulers. A Google search on ‘pain charts’ will show you a variety. Some have basic descriptions on them, like ‘Mild pain’ at 2 and ‘Very severe pain’ at 8. The advantages are that it is a quick way to establish the need for painkillers. Anything from 4 upwards grants consideration. It also gives a point of reference to find out if the medication has worked. It can easily be performed by anyone on the team. Frequently students get landed with recording the score. On the other hand it is very limited, and leaves a lot of room for interpretation. How is anyone to know how to score their pain? The usual reply to that is that any answer is correct as it is entirely subjective anyway, so, ‘Go with how you feel.’ I would argue that if the intention is as described above, that is justifiable. For patients who have been subjected to medical gaslighting this is particularly hard, though. They have learnt to doubt their inner compass when it comes to their health, and their experience of pain and any other symptom. They discovered that being honest leads to ridicule and disbelief. Also, it stands to reason that chronic pain sufferers are likely to rate pain differently than those for whom it is a rare occurrence. It helps when more context is given about the interpretation and what is expected. Only, there seems to be confusion about what that should be. Depending on place and person, the guidelines vary. A 10 can be seen as the worst pain you have ever had or the worst pain you can imagine, for example. The second is likely to be higher. And by that measure, how does the 10 of someone whose worst pain was when they stubbed their toe against a coffee table compare to that of someone who was once severely injured? There are inherent problems with quantifying qualitative information, anyway. As long as it is a case of comparing higher and lower within one individual situation, it should be fine. The natural tendency is to start applying math, though. Is a level 9 three times as painful as a 3? And if your groaning knee gets a 2 whilst the headache you have at the same time warrants a 6, does that make an 8 in total, or a 4 as average? Some scales give detailed descriptions of what each score means. An 8 for example might be described as, ‘So bad it keeps you awake’. Again, there are many and they each fill in the details in their own way. A 10 can be screaming with pain in one, and having turned completely silent in another. It is clear then that there is value in seeing these evaluation tools as an opening to a conversation, one in which the professional guides the patient into and through their own description of what they are facing. That takes skill and time. There are other tools that can aid this process. Lists of words that can apply to pain exist, as do assessments based on observation. Gingerbread figures can be used to indicate place, severity, type and recurrence using distinct colours and markings. The same Google search will bring you to this article which presents a collection of them. There is indeed a lot more to say than how much it hurts. The better the patient can express what they are going through, the more understood they are likely to feel. In terms of the trust that has been damaged in gaslit patients, this can be vital to establishing a therapeutic relationship. Again it is clear how important context is. In an emergency room speed is of the essence, whereas a pain clinic requires detailed understanding. Taking the time to explain that is a worthwhile investment. A therapist of mine pointed out to me that in the Western world we tend to describe pain in combative terms. We will say our head is about to explode, we are being kicked in the gut, it feels like a knife is cutting into us. In the East, apparently, more creative and peaceful terminology is used, ‘A bear is dancing in my head’. I bore that in mind when writing my book, and concentrated on how each episode felt specifically. It led me to descriptions like Lilliputians appeared to be playing on a rusty seesaw in my lower belly, a cablecart travelled through my body, and sharp, sour liquid seeping into my muscles, joints and organs. Picturing what it feels like, makes it possible to put words to it that others grasp quickly. Perhaps if we learnt to do that more often, our vocabulary would expand as we become more comfortable with its use. That would save time in coming to clarity. If this was normalised, patients with a medical history that includes gaslighting, would have less reason to be afraid when voicing what they feel in their bodies. The gap between chronic and acute illness would naturally close. What are your thoughts? The talk I refer to was held in Dutch. If anyone would like me to host a chat about this subject in English, I would be very happy to.
Back to Blog
Normal.14/4/2024 
It is a shame that it takes many chronically ill patients so much time and self-advocacy to get a solid team together to support their health and well-being. Once it is in place, the fear and dread remain at the idea of any changes. New people may bring back the old experiences.
The bigger and stronger the choir, the more it can allow for a false note from one person, or a pause for breath by another. It is worth the investment, in my opinion. On the whole I now have a brilliant team. By its mere existence it creates pressure on new professionals joining to step up to the plate. It appears to have an internal safety mechanism, which makes it easier on me, leaving a little more energy to spend on things that ensure my quality of life in other ways. Lately, of course, most of that has gone to my book ‘Recognise ME’. To a lay person it may sound odd when I say what a relief it was to hear my GP almost finishing the sentence she was inadvertently about to utter, ‘in other circumstances, I might say chances of this happening are slim, but you are not no…’ I laughed, as did my husband and the doctor joined in. It is a wonderful acknowledgement, rather than an insult, when a physician states I am not normal, if it means they are prepared to expect the unexpected. This was the case, as I consulted her about the ongoing abdominal issue. The pain is still at a level at which it was initially assumed to be due to kidney stones. That should give some idea as to what I have been going through for weeks now. I have an appointment with my favourite gastro- enterologist at the end of May. It has been years since I saw him. He has moved to a university hospital further away and become a professor there. He was always clued up on my combination of conditions, and willing to work in tandem with me. He is worth the wait and the drive. The GP and I were speculating what could be the cause. We were trying to decide how to deal with it until we know more. Tears rolled as I expressed my fear at having countless investigations performed again, only for the cause to remain a mystery until in years to come, by accident, proof that there is a physical issue explaining it all is found. Together we agreed to try some medication that helped in a similar situation over 20 years ago. Only, it turns out it is off the market at the moment. Honestly, if any of you happen to have a spare packet of Lynestrenol (a.k.a. Orgametril) lying about, please send it to me. Equally, if you know where I can get one (preferably, legally…), please let me know. Meanwhile I have tried to identify patterns in response to lifestyle, but it is becoming increasingly clear that gives me precious little control over the symptoms. Painkillers are, again, the answer. I am trying to stop myself from seeing this as a failure, after having managed to reduce my heavy schedule to almost zero after my neck operation. Thankfully my memoir and its launch have offered distraction. It is, also again, a balancing act and a case of prioritising to get done what needs doing. It is pretty much as Justine Steckling (a.k.a. Bipolar Beauty) and I discussed in relation to our recent interview. The fact that we look like we are managing, despite both claiming to be in severe pain is due to being well-practised. It has reminded me of a lecture on optimum stress levels, which was part of my OT training. With the support of my family, my publisher and my friends, I am managing to keep the pressure at the exact point where it motivates me to perform at my best, accepting that that best is affected by the circumstances. Exciting things are happening. We are set to go to the UK mid-May for the launch and to give a few talks, including a couple for the University of Leeds. I will be speaking to ME-patients in New Zealand online, I believe that is in the summer. The pre-publication version is almost ready, a press release has been written, the official photographs from the shoot have been received, and we are set to start receiving pre-orders soon. If you would like to be kept informed and receive invitations to any upcoming events, make sure you are on my mailing list! |
 RSS Feed
RSS Feed
